ABDOMINAL WALL HERNIAS
Umbilical Hernias
Umbilical hernias are the most common type of ventral hernias and are usually asymptomatic.
They are habitually congenital,
resulting from incomplete closure of the abdominal wall after ligation of the umbilical cord.
In adults they appear generally in context of multiple pregnancies,
ascites,
obesity,
abdominal masses or chronic increased abdominal pressure.
The herniated sac usually contains the greater omentum or bowel loops,
that can be incarcerated,
causing symptoms of intestinal obstruction and local tenderness (Fig.1).
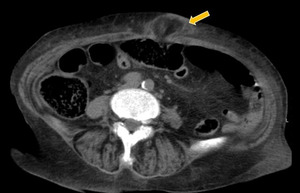
Fig. 1: Axial unenhanced CT scan shows an umbilical hernia. Thickening and edema of the fat planes suggesting acute complications (inflammation/ischemia).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Paraumbilical Hernias
Paraumbilical hernias arise in the midline near the umbilicus.
They are commonly associated with diastasis of the rectus abdominis muscles (Fig.
2).
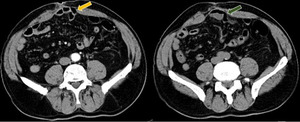
Fig. 2: Axial CT scans show paraumbilical hernias (arrows). They are usually associated with diastasis of the rectus abdominis muscles.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Hypogastric Hernias
Hypogastric hernias arise below the umbilicus in linea alba (Fig.
3).
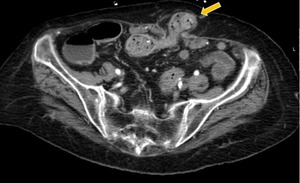
Fig. 3: Axial CT scan depict an uncomplicated hypogastric hernia containing bowel loops.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Epigastric Hernias
Epigastric hernias arise in linea alba between the umbilicus and the xyphoid process.
When associated with pain,
it can simulate peptic ulcer or gallbladder illness (Fig.
4).
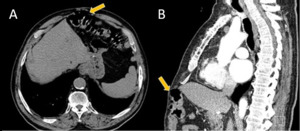
Fig. 4: Axial unenhanced (A) and sagittal enhanced CT (B) show epigastric hernias (arrows) with only a portion of the bowel wall in the hernial sac (Richter´s hernia).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Spigelian Hernias
Spigelian hernias are related to a congenital weakness in the posterior layer of the transverse fascia,
near the junction of semilunar line and arcuate line.
These hernias are uncommon and the diagnosis can be difficult,
because they are often interparietal and extend between muscular or fascial layers of the anterior abdominal wall (Fig.
5).
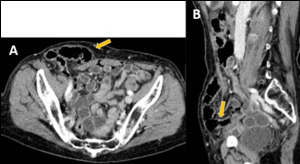
Fig. 5: (A) Axial and (B) sagittal enhanced CT scans depicting a right Spigelian hernia. The hernial sac contains portion of the sigmoid colon without signs of complications.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Lumbar Hernias
Lumbar hernias are located below the 12th rib and above the iliac crest.
They occur related to defects in the lumbar muscles or the posterior fascia,
usually secondary to surgery (e.g.
kidney surgeries) or trauma.
- Superior Lumbar Hernias (Grynfelt-Lesshaft Hernias)
Superior lumbar hernias arise in the superior lumbar triangle bordered anteriorly by the internal oblique muscle,
the 12th rib superiorly,
and the erector spinal muscle posteriorly (Fig.
6).
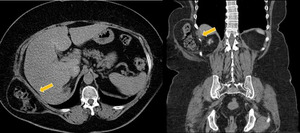
Fig. 6: Axial and coronal CT scan showing a right superior lumbar hernia containing the colon's hepatic flexure. The patient was asymptomatic and no signs of complication were seen.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
- Inferior Lumbar Hernias (Petit Hernias)
Inferior lumbar hernias occur through the inferior lumbar triangle bordered anteriorly by the external oblique muscle,
the 12th rib superiorly,
and the erector spinal muscle posteriorly.
Incisional Hernias
Incisional hernias occur through defects related to prior abdominal surgeries (Fig.
7,
Fig.
8).
They usually represent a delayed complication.
Symptoms are present within the first 4 months after surgery.
The risk of an incisional hernia is higher in vertical incisions and after wound infections with subsequent dehiscence.
Predisposing factors include old age,
malnutrition,
malignancy,
pregnancy,
ascites,
chronic pulmonary diseases and obesity.
Paraestomal Hernias are considered a subtype of incisional hernia.
They occur adjacent to a stoma and are particularly difficult to detect at physical examination (Fig.
9).
Fig. 7: Incisional hernia containing small bowel loop. There were no signs of incarceration and the hernia was manually reducible.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
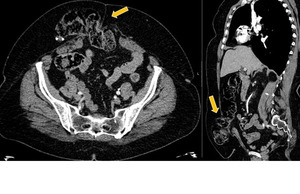
Fig. 8: Axial and sagittal enhanced CT scans show a large defect on the abdominal wall at the location of a previous surgery. The herniated sac contains a segment of the transverse colon. No signs of acute complications were seen.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
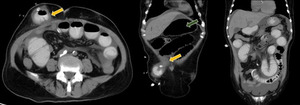
Fig. 9: Peritoneal dialysis catheter related hernia (arrows).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Groin hernias
-Inguinal Hernias
Inguinal hernias represent the most common type of abdominal hernia,
more commonly found in males.
They can be distinguished by its relation with the epigastric vessels.
Direct hernias occur medial to the inferior epigastric vessels,
and are usually acquired,
resulting from a weakness of the transversal fascia in Hesselbach’s triangle.
The peritoneal sac protrudes through the inguinal canal and emerges at the external inguinal ring (Fig.
10).
The inguinal canal is usually compressed or displaced (“lateral crescent sign”).

Fig. 10: Right inguinal hernia (arrow). Direct type.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Indirect hernias are more common than direct hernias,
and the majority occurs in men due to persistence of the process vaginalis during testicular descent (Fig.
11).
They arise lateral and superior to the inferior epigastric vessels and lateral to the Hesselbach’s triangle.
In men,
they enter the canal anterior to the spermatic cord and may extend to the external inguinal ring into scrotum (Fig.
12).
In women,
they tend to follow the round ligament into the labia majora.
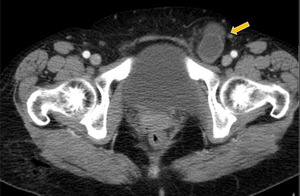
Fig. 11: Left inguinal hernia (arrow). Indirect type.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
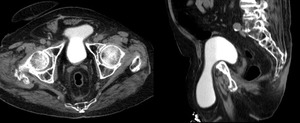
Fig. 12: Inguinoscrotal hernia, with herniation of the bladder through the scrotum.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Femoral hernias arise inferior of the course of the inferior epigastric vessels and medial to the common femoral vein (Fig.
13).
They are more frequent in women.
Acute complications are more frequently than in inguinal hernias due to the narrower orifice.
They regularly compress the femoral vein.

Fig. 13: Right femoral hernia, containing ascitic fluid.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Other Hernias
Obturador Hernias are rare,
primarily found on women with previous pregnancy or significant weight loss.
The peritoneal sac and its contents protude between the external obturador and pectineal muscles (Fig.
14).
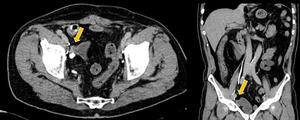
Fig. 14: Obturator hernia. Axial and coronal CT scans show a small right obturator hernia (arrows).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Traumatic Hernias are related to high energy traumas,
usually requiring surgical correction.
They are most common in locations with relative anatomic weakness,
the lumbar region and the lower abdomen.
Interparietal Hernias or interstitial hernias consists of a herniation that not exit the subcutaneous tissue,
usually located in the fascial planes between the abdominal wall muscles (Fig.
15).
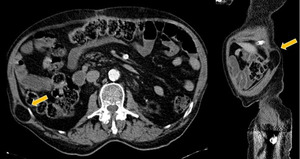
Fig. 15: Interparietal hernia. Axial and sagittal CT scans demonstrating a right posterior interparietal hernia containing only peritoneal fat.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
COMPLICATIONS
Incarceration refers to an irreducible hernia due to narrowing of hernia orifice.
Early detection is important to prevent complications such as obstruction,
inflammation or ischemia.
The presence of free fluid in the herniated sac,
bowel wall thickening or luminal dilatation suggests incarceration (Fig.
16).
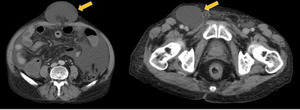
Fig. 16: Incarcerated umbilical hernia in a 66 years-old patient with acute abdominal pain. Axial enhanced CT scans shows an umbilical hernia incarcerated with ascitic fluid.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Bowel obstruction
Abdominal wall hernias are the second leading cause of small bowel obstruction.
Dilated bowel proximal to the hernia and normal or reduced caliber of the bowel distal to the obstruction are the key imagiologic features (Fig.
17).
Other ancillary sign include fecalization of small bowel contents proximal to the obstruction.
Colonic obstruction caused by an abdominal wall hernia is rare.
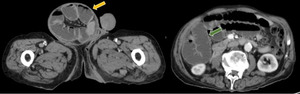
Fig. 17: Small bowel obstruction. 72 years-old patient presented with an inguinoscrotal mass and acute abdominal pain. Axial enhanced CT scans show herniation of small bowel loops through the inguinal canal (yellow arrow), causing intestinal obstruction with dilated loops (green arrow).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
DIAPHRAGMATIC HERNIAS
Diaphragmatic hernias are defined as either congenital or acquired defects in the diaphragm.
Congenital
There are two main types of congenital diaphragmatic hernia that usually occur on the left side (80%) of the diaphragm:
- Bochdalek hernia: most common (95%),
located posterolaterally and usually present in infancy (Fig.
18).
- Morgagni hernia: smaller,
anterior and presents later in life,
through the sternocostal angles (Fig.
19).
Acquired
There are a variety of aetiologies for acquired diaphragmatic hernias that usually occur in adulthood,
namely traumatic diaphragmatic rupture,
hiatus hernia (Fig.
20),
and iatrogenic.
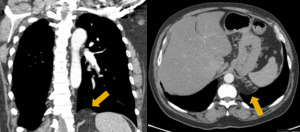
Fig. 18: Left Bochdalek hernia (arrows).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
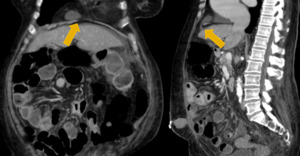
Fig. 19: Right Morgagni hernia (arrows).
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT

Fig. 20: Bulky hiatal hernia, containing transverse colon, stomach and greater omentum.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
INTERNAL HERNIAS
PARADUODENAL HERNIAS
Left Paraduodenal Hernias are entrapments of the small intestine into the fossa of Landzert,
an unusual congenital peritoneal fossa behind the descending mesocolon that is present in 2% of individuals.
At CT,
intestinal loops with a saclike appearance are seen in the left anterior pararenal space.
The inferior mesenteric vein and ascending left colic artery are landmarks situated at the anteromedial edge of the fossa of Landzert.
In the event of a left paraduodenal hernia,
the inferior mesenteric vein is observed anterior and medial to the hernia orifice and entrapped intestine.
Right Paraduodenal Hernia usually involves the fossa of Waldeyer and occur most frequently in the setting of a nonrotated small intestine.
The fossa of Waldeyer is located inferior to the third portion of the duodenum,
behind the root of the small bowel mesentery,
and extends rightward and downward into the ascending mesocolon.
Landmarks for the hernia orifice at multidetector CT are the superior mesenteric artery and superior mesenteric vein that run along the anteromedial free edge of the fossa (Fig.
21).
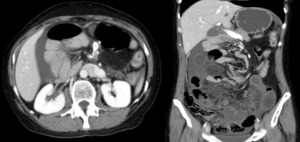
Fig. 21: Right paraduodenal hernia in a 53-year-old female with sudden abdominal pain - Contrast-enhanced CT scan shows a saclike fluid-filled bowell loops and the encapsulated bowel loops herniated through the fossa of Waldeyer. The superior mesenteric artery is displaced anteriorly.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
SMALL BOWEL MESENTERY–RELATED HERNIA
Transmesenteric Hernia is the most common one,
and affects both peritoneal layers.
Although displacement of the main mesenteric trunk to the right has been reported as a useful CT finding,
this subtype does not show a saclike appearance and has no key vessels,
making it difficult to distinguish from other causes of small-howell obstruction (Fig.
22).
Furthermore,
transmesenteric hernias tend to be complicated by volvulus.
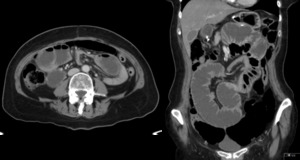
Fig. 22: Transmesenteric hernia in a 67-year-old female - Contrast-enhanced CT scan shows dilated and fluid-filled small bowel loops and crowded and stretched vessels. No sac is observed. On surgery it was demonstrated incarcerated intestine through a defect in the mesentery of the ileum.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
Intramesenteric Hernias are less frequent and predominantly occur in children.
Either one of the two peritoneal layers can be affected.
CT findings include a cluster of small bowel encapsulated within a hernia sac and displacement of the superior mesenteric artery and superior mesenteric vein.
GREATER OMENTUM–RELATED HERNIA
Transomental hernia are a closed-loop intestine without a saclike appearance,
located in the most anterior portion of the peritoneal cavity,
because the direction of a transomental hernia is usually posterior to anterior (Fig.
23).
Omental branches of the left and right gastro-omental vessels are landmarks that run inside the greater momentum and run vertically around the hernia orifice.

Fig. 23: Transomental hernia in a 51-year-old man with acute diffuse abdominal pain. Contrast-enhanced CT scan shows dilated and fluid-filled closed bowel loops and engorged and crowded mesenteric vessels at the hernial orifice.
References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT
FORAMEN OF WINSLOW HERNIAS
Foramen of Winslow hernias account for 8% and are the most common type of lesser sac hernia.
They are herniations in which the viscera enter the lesser sac through the foramen of Winslow and are congenital.
The most commonly involved viscus is the small bowel,
but the terminal ileum,
cecum,
ascending colon,
transverse colon,
and gallbladder can also be involved at a rate about 25%.
The presence of herniated viscera in the lesser sac,
in a “beak” shape pointing toward the foramen of Winslow,
is observed at multidetector CT.
When the small or large intestine is involved,
the presence of mesenteric vessels between the inferior vena cava and portal vein is also diagnostic.
TRANSVERSE MESOCOLON-RELATED HERNIA
Transverse mesocolon-related hernia are herniations through or into an abnormal defect
in the transverse mesocolon,
in which the herniated viscera displace the transverse colon anteriorly and inferiorly.
They are uncommon without a history of surgery,
however an increasing number of cases have been reported after Roux-en-Y anastomosis surgery.
There are two subtypes of transverse mesocolon–related hernias according to the degree of the defect: (a) transmesenteric,
if a complete defect in the transverse mesocolon is present; or (b) intramesentbric,
if the defect is only in the posterior peritoneal layer of the transverse mesocolon,
and the herniated viscera are trapped within the transverse mesocolon.
PERICECAL HERNIA
Pericecal hernias account for 13% of all internal hernias.
They are herniations into an unusual recess near the cecum,
including the superior ileocecal recess,
inferior ileocecal recess,
retrocecal recess,
and paracolic sulci.
In addition to these congenital recesses,
acquired conditions such as adhesion may cause a pericecal hernia.
CT findings of pericecal hernia are characteristic.
A saclike appearance is seen,
and the hernia sac displaces the cecum and ascending colon anteriorly or medially.
SIGMOID MESOCOLON–RELATED HERNIA
Sigmoid mesocolon-related hernias account for 6% of all internal hernias and can be classified into three subtypes: transmesosigmoid,
intramesosigmoid,
and intersigmoid.
Transmesosigmoid and intramesosigmoid hernias are herniations through or into an abnormal defect in the sigmoid mesocolon.
A transmesosigmoid hernia is a herniation through a complete defect in both of the peritoneal layers of the sigmoid mesocolon.
An intramesosigmoid hernia is a herniation into an abnormal defect in only one peritoneal layer,
making the herniated viscera trapped in the sigmoid mesocolon.
On the other hand,
an intersigmoid hernia involves the intersigmoid fossa,
a congenital retroperitoneal fossa present in 70% of individuals,
located just above and behind the apex of the root of the sigmoid mesocolon.
At CT,
the hernia orifice can be observed between the sigmoid colon and the left psoas major muscle in all three subtypes.
The key to diagnosis of a transmesosigmoid hernia is absence of a saclike appearance,
while intramesosigmoid and intersigmoid hernias show a saclike appearance.
PELVIC INTERNAL HERNIA
Broad Ligament Hernia is a herniation through or into an abnormal opening in the broad ligament of the uterus and account for 4-5% of all internal hernias.
80% of broad ligament defects occur in multiparous women.
The most common hernia content is the small intestine.
They can be classified into two subtypes,
according to the degree of the defect.
The fenestra type is the most common and it is a herniation through both peritoneal layers of the broad ligament.
No hernia sac is present,
and the herniated intestine is located lateral to the uterus in the pelvic cavity.
The pouch type is a herniation into a defect in only one of the two peritoneal layers of the broad ligament and manifests as herniated viscera within a sac trapped in the parametrium.
ROUX-EN-Y ANASTOMOSIS–RELATED HERNIA
Reconstruction of a Roux-en-Y anastomosis is one of the common and increasing procedures in gastric surgeries.
Internal hernia is a major complication of this anastomosis and results more commonly after laparoscopic gastric bypass surgery than open surgery.
Three subtypes of transmesenteric-type hernias can occur: transmesocolic,
jejunojejunostomy mesenteric,
and Petersen hernias.
At CT,
the anatomy in patients who have undergone Roux-en-Y gastric bypass surgery is complex.
In addition,
Roux-en-Y anastomosis-related hernias without intestinal obstruction are sometimes observed.
CT signs that suggest this diagnosis are mesenteric swirl,
clustered small bowel loops,
the “mushroom” sign (a mushroom-shaped mesenteric root between the superior mesenteric artery and the distal mesenteric arterial branch),
the “hurricane eye” sign (distal tubular mesentery with surrounding small bowel loops),
a small bowel loop behind the superior mesenteric artery,
abnormal position of the jejunojejunostomy,
and “weeping mesentery” (edematous mesentery with enlarged lymph nodes).

. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
. They are usually associated with diastasis of the rectus abdominis muscles. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")

 and sagittal enhanced CT (B) show epigastric hernias (arrows) with only a portion of the bowel wall in the hernial sac (Richter´s hernia). References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
 Axial and (B) sagittal enhanced CT scans depicting a right Spigelian hernia. The hernial sac contains portion of the sigmoid colon without signs of complications. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")



. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
. Direct type. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
. Indirect type. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")


. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")


, causing intestinal obstruction with dilated loops (green arrow). References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")
. References: Department of Radiology, Centro Hospitalar São João, Faculdade de Medicina da Universidade do Porto – Porto/PT")



